
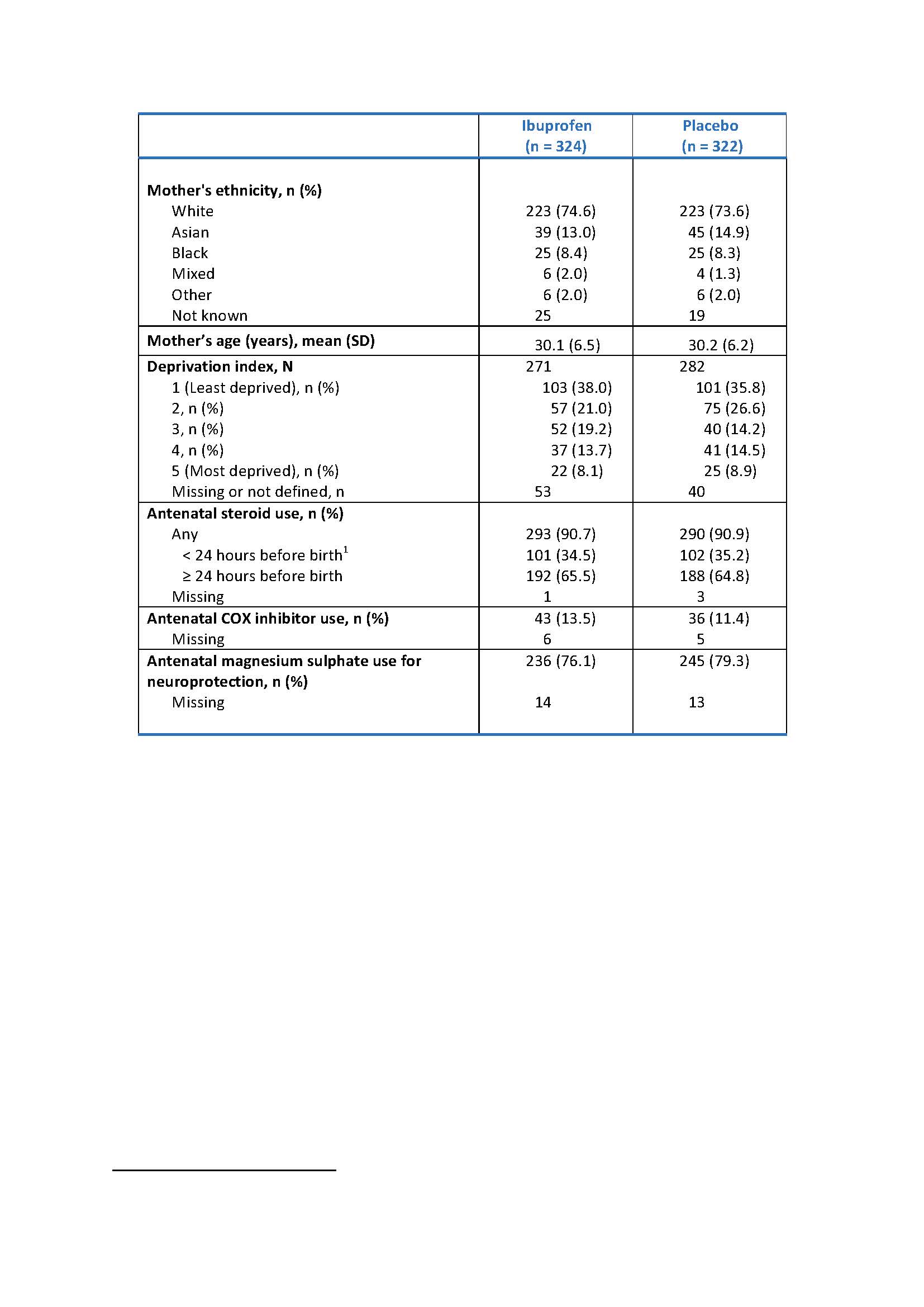
image: Table 1a - Maternal baseline characteristics Doses would usually be 24 hours apart, so < 24 hours before birth suggests only one dose was taken view more
Credit: Department of Engineering, Durham University, United Kingdom
DENVER, April 22, 2022 – A randomized controlled trial evaluates if selective early treatment of patent ductus arteriosus reduces death or bronchopulmonary dysplasia at 36 weeks in extreme preterm babies. Findings from the study will be presented during the Pediatric Academic Societies (PAS) 2022 Meeting, taking place April 21-25 in Denver.
The management of patent ductus arteriosus continues to be a clinical conundrum in extremely low gestational age newborns. Presence of a patent ductus arteriosus at 72 hours after birth in extremely low gestational age newborns is associated with an increased risk of death and complications of prematurity. Functional echocardiography is increasingly used to assess the haemodynamic impact of patent ductus arteriosus and can be used in the first three days after birth to select babies with a large pre-symptomatic patent ductus arteriosus.
Baby-OSCAR trial is a UK multi-center placebo-controlled masked randomized clinical trial in extremely low gestational age newborns (23+0 to 28+6 weeks gestational age). The objective of the study was to evaluate whether early targeted treatment of a large patent ductus arteriosus (diagnosed by functional echocardiography) with ibuprofen within 72 hours of birth improves short term health outcomes of death or moderate to severe bronchopulmonary dysplasia at 36 weeks post-menstrual age.
Researchers found no evidence of a reduction in death or moderate to severe bronchopulmonary dysplasia with early selective treatment of a large patent ductus arteriosus with ibuprofen within 72 hours of birth in extreme preterm infants.
“The aim of Baby-OSCAR trial was to find out whether or not a large patent ductus arteriosus in extreme preterm babies should be treated with ibuprofen within 72 hours of birth,” said Samir Gupta, MD, chief investigator and professor of neonatology at Durham University, UK. “Ibuprofen is a non-steroidal anti-inflammatory drug that is commonly used for pain relief in adults. Patent ductus arteriosus is a condition that is caused by a blood vessel called the ductus arteriosus staying open after a baby’s birth. During pregnancy, the ductus arteriosus allows blood from the baby’s heart to flow to the mother’s placenta to get oxygen, bypassing the baby’s lungs. Soon after birth the ductus should close to allow blood to flow to the baby’s own lungs to get oxygen. However, in extreme preterm babies the ductus often takes a long time to close on its own and this can lead to a variety of complications. Clinicians are unsure if early treatment should be offered to extreme preterm babies to close the patent ductus arteriosus and reduce the risks of complications, or whether it would be better to wait and see if the ductus will close on its own.”
Dr. Gupta added: “In the Baby-OSCAR trial, extreme preterm babies were screened in first 72 hours with echocardiography and those with a large patent ductus arteriosus meeting inclusion criteria were randomized to either treatment with i.v. ibuprofen or placebo. About ~4,000 extreme preterm babies were screened in 32 tertiary neonatal intensive care units with echocardiography in the UK, and 653 of them were randomized after parental consent. The results on short term outcomes till discharge are presented. Babies are currently being followed up to two years corrected age for assessment of neurodevelopment and respiratory morbidity and prospective health economic evaluation is conducted.”
“The short term outcomes demonstrated no evidence of benefit of early targeted treatment with ibuprofen within 72 hours of birth compared to placebo in extreme preterm babies with a large patent ductus arteriosus on death or moderate/severe bronchopulmonary dysplasia at 36 weeks postmenstrual age. There were no significant differences in other complications of prematurity, however, babies treated with ibuprofen had reduced the risk of an open patent ductus arteriosus at three weeks of age and significantly less need for surgical treatment for a symptomatic patent ductus arteriosus.”
The trial was funded by National Institute for Health Research – Health Technology Assessment (NIHR-HTA) program, UK, and managed by National Perinatal Epidemiology Unit (NPEU) at Oxford University, UK.
Dr. Gupta will present “Does Selective Early Treatment of Patent Ductus Arteriosus (PDA) Reduce Death or Bronchopulmonary Dysplasia(BPD) at 36 weeks in Extreme Preterm Babies? A Randomised Controlled Trial (Baby-OSCAR Trial)” on Saturday, April 23 at 2 p.m. MDT. Reporters interested in an interview with Dr. Gupta should contact PAS2022@piercom.com.
The PAS Meeting connects thousands of pediatricians and other health care providers worldwide. For more information about the PAS Meeting, please visit www.pas-meeting.org.
###
About the Pediatric Academic Societies Meeting
The Pediatric Academic Societies (PAS) Meeting is the premier North American scholarly child health meeting. The PAS Meeting connects thousands of pediatricians and other health care providers worldwide. The PAS Meeting is produced through a partnership of four pediatric organizations that are leaders in the advancement of pediatric research and child advocacy: American Pediatric Society, Society for Pediatric Research, Academic Pediatric Association and American Academy of Pediatrics. For more information, please visit www.pas-meeting.org. Follow us on Twitter @PASMeeting, Instagram PASMeeting and #PAS2022, and like us on Facebook PASMeeting.
---
Abstract: Does Selective Early Treatment of Patent Ductus Arteriosus (PDA) Reduce Death or Bronchopulmonary Dysplasia(BPD) at 36 weeks in Extreme Preterm Babies? A Randomised Controlled Trial (Baby-OSCAR Trial)
Topic
Neonatal Clinical Trials
Presenting Author
Samir Gupta, MD DM FRCPCH FRCPI
Organization
Department of Engineering, Durham University, United Kingdom
Background
The management of PDA continues to be a clinical conundrum in extremely low gestational age newborns (ELGANS). Presence of a PDA at 72 hours after birth in ELGANS is associated with an increased risk of death and complications of prematurity. Functional echocardiography (fEcho) is increasingly used to assess the haemodynamic impact of PDA & can be used in the first 3 days after birth to select babies with a large pre-symptomatic PDA.
Objective
To evaluate whether early targeted treatment of a large PDA (diagnosed by fEcho) with ibuprofen within 72 hours of birth improves short term health outcomes of death or moderate to severe BPD at 36 weeks post-menstrual age (PMA).
Design/Methods
Baby-OSCAR trial is a UK multi-centre placebo-controlled masked randomised clinical trial in ELGANS (23+0 to 28+6 weeks gestational age). With parental consent, eligible babies admitted to tertiary NICU were screened using fEcho. Babies with a large PDA on echo, (diameter >1.5mm and with a pulsatile or growing pulse wave Doppler ductal flow pattern), were randomised in the first 72 hours after birth. A central web randomisation with minimisation was used to allocate treatments. Babies received either i.v. ibuprofen at dose 10-5-5 mg/kg 24 hours apart or matched placebo (0.9% normal saline). The primary outcome was a composite of death or moderate to severe BPD at 36 weeks PMA. The trial was funded by the UK National Institute for Health Research (NIHR). Ethical approval was obtained from East Midlands Research Ethics Committee. Statistical analysis by intention-to-treat was performed using Stata 17®.
Results
A total of 3848 ELGANS were screened with fEcho from 32 tertiary NICU in the UK from July 2015–December 2020. Of these, 653 infants were randomised; 326 to ibuprofen & 327 to placebo. Maternal and infant baseline characteristics were broadly similar between the study groups (Table 1). The median size of the PDA was 2.2 mm in both groups. The primary outcome event rate in the ibuprofen and control groups was 220/318 (69.2%) and 202/318 (63.5%) respectively; adjusted risk ratio 1.09 (95% CI 0.98 to 1.20); p=0.104. There was no evidence of differences in the secondary outcomes, except less need for surgical ligation (2.8% vs 9.6%; p< 0.001) and higher proportion of closed / non-significant PDA at ~3 weeks age (55.5% vs 37%; p< 0.001) in ibuprofen compared to placebo group (Table 2).
Conclusion(s)
We found no evidence of a reduction in death or moderate to severe BPD with early selective treatment of a large PDA with ibuprofen within 72 hours of birth in extreme preterm infants.
Tables and Images
Table 1a - Maternal baseline characteristics
Doses would usually be 24 hours apart, so < 24 hours before birth suggests only one dose was taken
Table 1a-Maternal baseline characteristics.jpg
{kind=link}
Table 1b - Infant's characteristics at trial entry
1 Including abnormally implanted placenta 2 +/- APH 3Nasal CPAP, nasal ventilation, humidified high flow nasal cannula therapy, or low flow oxygen ≥ 1.1L/min 4In room air, low flow oxygen < 1.1L/min, or ambient oxygen)
Table 1b-Infant's characteristics at trial entry_Page_1.jpg
.jpg){kind=link}
Table 2 - Secondary outcomes (Tested)
1 Adjusted for size of PDA at randomisation, gestational age at birth, age at randomisation, sex, multiple birth, mode of respiratory support at randomisation, receiving inotropes at time of randomisation, and centre as a random effect, and clustered by siblings to account for correlation between multiple births 2 With ventricular dilatation or intraparenchymal abnormality 3 In at least one eye 4 Fresh blood in endotracheal tube with increase in respiratory support 5 Confirmed by radiography and/or histopathology 6For descriptive purposes only
Table 2- Secondary outcomes (Tested).jpg
.jpg){kind=link}
Method of Research
Randomized controlled/clinical trial